It’s the foundation of medicine. Treat the sick, with treatments that work, is far better policy for public health than constant vaccine jabs for everyone. Or even 1 jab for everyone for this disease.
Treating the sick, the foundation of medicine, has been hijacked by a pharma industrial complex that is not satisfied with selling medicines for the sick. Their agenda for decades has been to pump their products into all people including healthy people, a much larger market.
Selling Sickness: How the World's Biggest Pharmaceutical Companies are Turning Us All into Patients
Thirty years ago, the head of the drug company Merck made some remarkably candid comments about his distress that his company's market was limited to sick people. Suggesting he would like Merck to be more like the maker of Wrigley's chewing gum, the CEO said it had long been his dream to make drugs for healthy people, to "sell to everyone." That dream now drives the marketing machinery of the most profitable industry on earth. From award-winning Ray Moynihan,—one of the world's top medical journalists—Selling Sickness reveals how widening the boundaries of illness and lowering the threshold for treatments is creating millions of new patients and billions in new profits. This in turn is driving up personal drug bills and threatening to bankrupt national health systems all over the world. As more and more ordinary life is "medicalized," the industry moves ever closer to being able to "sell to everyone."
I was just telling a friend, a Swede, about things that have changed in my lifetime, 55 years, in the United States. When I was a kid in the 60s and 70s, we took, I don’t know, maybe 6 or 8 vaccine injections. For kids born today, if they follow the CDC recommended vaccine schedule, they’ll have 78 injections from birth to age 18.
HA! 78 injections! Where’d you hear that? Some blog?
- (yelled out with some volume)
Well, I said, it’s from the horse’s mouth, from the CDC.gov website.
So?
Well, that’s the official source. CDC is the authority.
I went the next day to the CDC site and checked again:
I counted 84 injections from birth to age 18. That does not include covid vaccine doses. So add those to the total:
I live in Sweden now, last 3 years, so I don’t get much exposure now to American media. And I don’t speak Swedish, so I don’t read or watch their news channels either. But there are plenty of serious Swedish data nerds and whatnot, writing in english. Tommy Lennhamn is a constant source of good analysis. His site here:
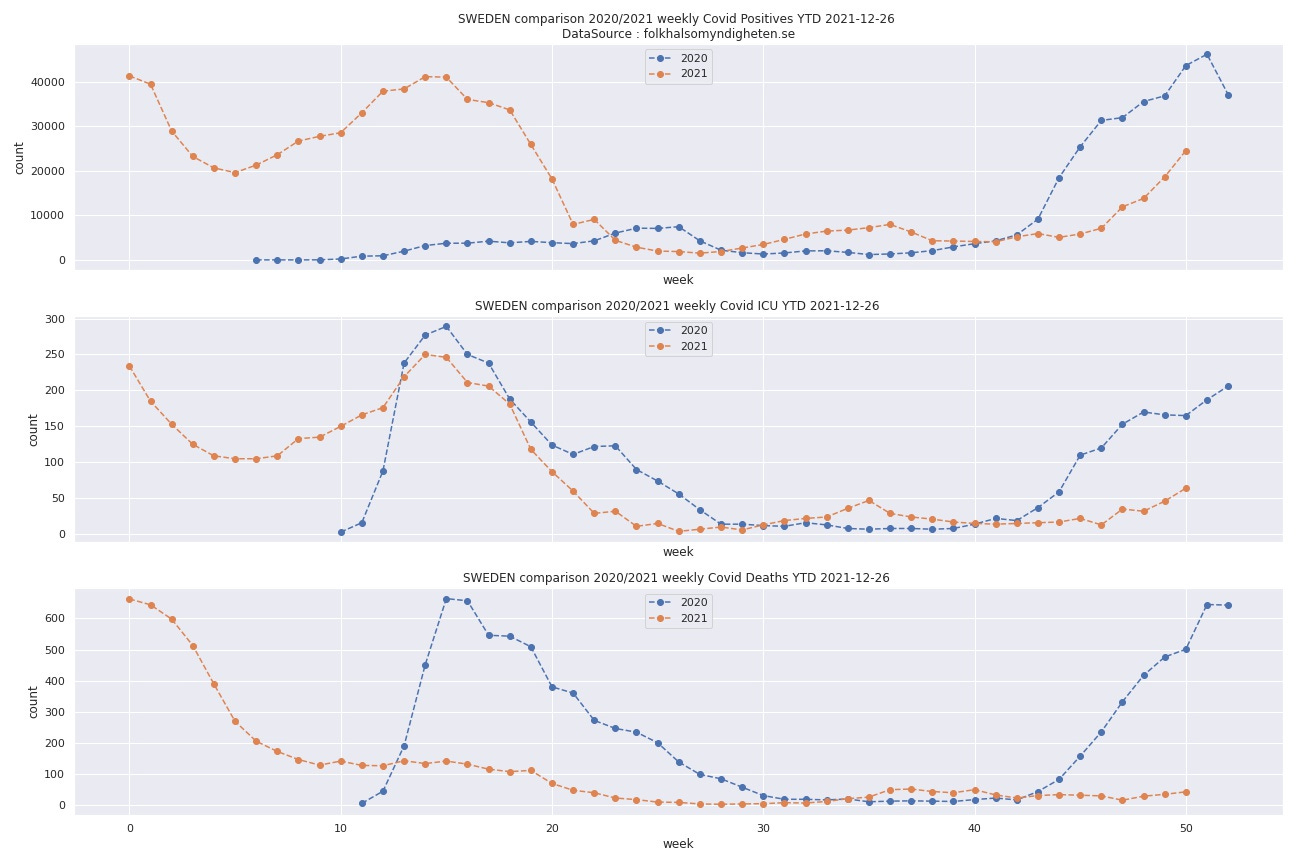
Notice Swedish ICU occupancy via covid for 2020 and 2021 (the middle graph). The sum of the figures for weekly Swedish ICU occupancy from covid are approximately 5000 patients total, the same in each year, 2020 (blue) and 2021 (orange):
So is that accurate? I eyeballed the Swedish Covid ICU graph and see about 5000 covid ICU patients in each year, 2020 and 2021. But, I’m eyeballing weekly ICU occupancy figures, and some patients are in hospital less than a week and some more than a week. So what are the actual number of covid patients in ICU in 2020 and 2021?
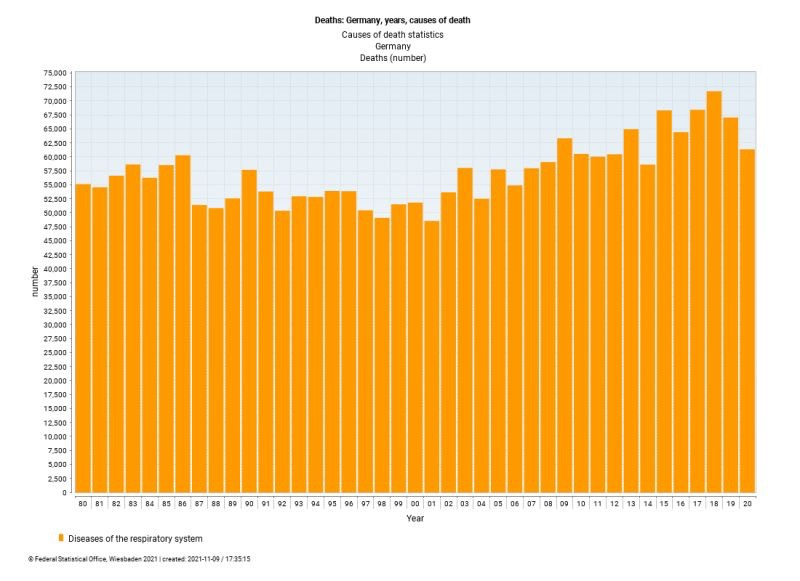
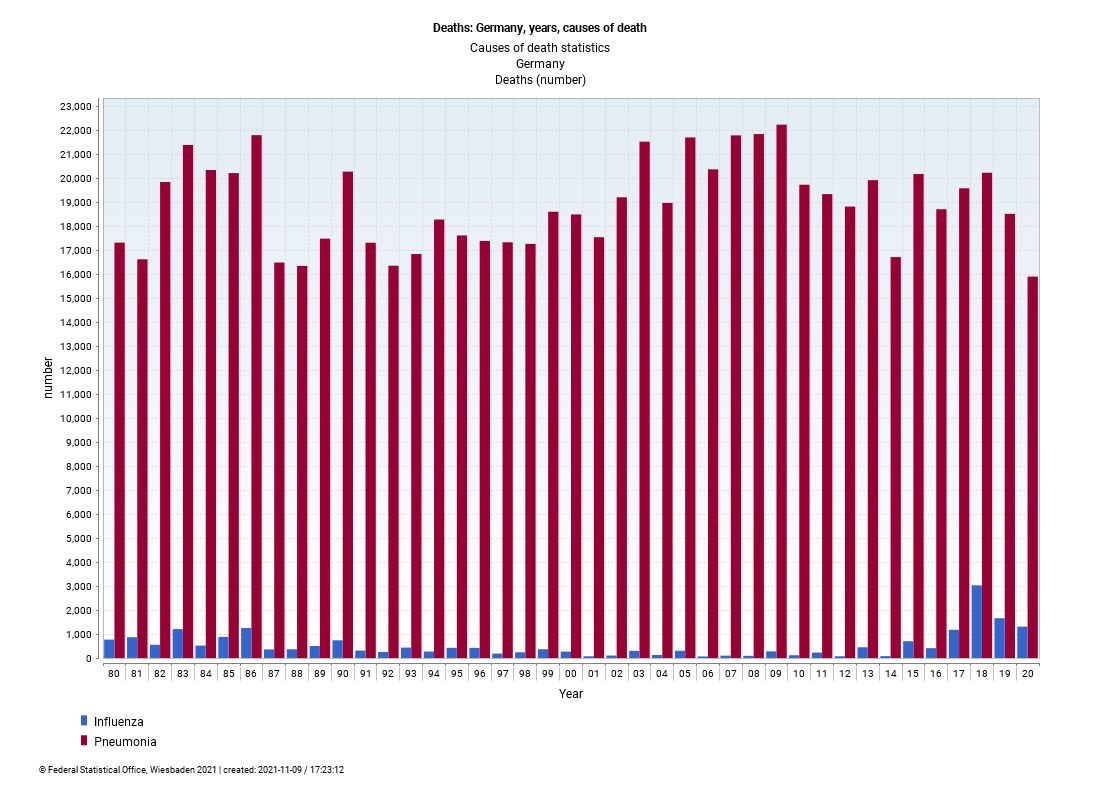
Now I’m wondering about hospitalization and ICU for “all respiratory diseases”. Recently I saw a graph of annual hospitalization and death from diseases of the respiratory system, absolute numbers in Germany since 1980.
4000 patients in ICU per year are the cause of understaffed hospitals in a country of 11 million?
11 million people should be injected with exotic pharma products because 4000 people are in ICU with respiratory illness?
How many of those 4000 would be in ICU anyway, if SARS-Cov-2 had never existed? Other viral respiratory contagions would not have been present? ICU admissions for severe respiratory disease would not have occurred at a similar rate?
On the occasion of the debate about the possible introduction of the general compulsory vaccination, we formulated seven scientific arguments which, in our opinion, prove that there is no reliable scientific basis for compulsory vaccination; From our point of view, this speaks clearly against the introduction of mandatory vaccinations.
We are very concerned about the possible decision to compulsory vaccination and therefore kindly ask for an independent scientific examination of the complex problem areas set out in the text before you make a decision on this matter.
If you have any questions, please do not hesitate to contact us ( autorengruppe@7argumente.de ) or contact us .
With respect for your responsible work and best regards,
the group of authors of the 7 arguments against compulsory vaccination
Download the 7 arguments against compulsory vaccination
Download PDF
The group of authors
Prof. Dr. Jessica Agarwal Prof. Dr. Dr. hc Kai Ambos Prof. Kerstin Behnke Prof. Dr. Andreas Brenner (CH) Prof. Dr. Klaus Buchenau Dr. phil. Matthias Burchardt Prof. Dr. med. Paul Cullen Prof. Dr. Viktoria Däschlein-Gessner Assoc.-Prof. Dr. theol. Jan Dochhorn Prof. Dr. Ole Döring Prof. Dr. Gerald Dyker Jun.-Prof. Dr. Alexandra Eberhardt Prof. Dr. Michael Esfeld (CH) Dr. Matthias Fechner Prof. Dr. Ursula Frost Prof. Dr. Katrin Gierhake Prof. Dr. Ulrike Guérot Prof. Dr. Lothar Harzheim Prof. Dr. Saskia Hekker Prof. Dr. med. Sven Hildebrandt Prof. Dr. Stefan Homburg Dr. Agnes Imhof Dr. René Kegelmann Prof. Dr. Martin Kirschner Dr. Sandra Kostner Prof. Dr. Boris Kotchoubey Prof. Dr. Christof Kuhbandner PD Dr. Axel Bernd Kunze
Prof. Dr. Salvatore Lavecchia Dr. Christian Lehmann Dr. hc theol. Christian Lehnert PD Dr. phil. Stefan Luft Prof. Dr. Jörg Matysik Dr. Christian Mézes Prof. Dr. Klaus Morawetz Prof. Dr. Gerd Morgenthaler Dr. Henning Nörenberg Prof. Dr. Gabriele Peters Dr. med. Steffen Rabe Prof. Dr. Markus Riedenauer Prof. Dr. Günter Roth Prof. em. Dr. Stephan Rist (CH) Prof. Dr. Steffen Roth Dr. med. Christian Schellenberg Prof. Dr. Andreas Schnepf Prof. Dr. Wolfram Schüffel Prof. Prof. Dr. med. Klaus-Martin Schulte, FRCS, FRACS Dr. Jens Schwachtje Prof. Dr. Harald Schwaetzer Prof. Dr. Henrieke Stahl Prof. Dr. Anke Steppuhn Prof. Dr. Wolfgang Stölzle (CH) Prof. Dr. Tobias Unruh Prof. Dr. Christin Werner Prof. Dr. Martin Winkler (CH) Prof. Dr. Christina Zenk
The 7 arguments
Overcoming the split : seven scientific arguments against compulsory vaccination and in favor of an open discourse
The corona pandemic has demanded a high human toll and great efforts in all areas of social life over the past two years. In quick succession, new ordinances and laws were passed, which large parts of the population responsibly supported. In the past few months, the political path has increasingly been geared towards vaccination of the entire population, which is mostly viewed as no alternative. This is currently culminating in the discussion of introducing a statutory vaccination requirement - both general and group-specific. The existing sanctions against “unvaccinated people” (and therefore also those whose vaccination certificate has expired) are to be expanded even further.
It is premature to pass a resolution on a statutory vaccination requirement. Because fundamental questions about the new vaccines have not been adequately clarified and are controversial in research. This includes in particular the duration and strength of the vaccination protection as well as the type, frequency and severity of the side effects. No such law should be based on controversial research questions.
The undersigned therefore take the position that a general or group-specific mandatory vaccination against SARS-CoV2 is not justifiable in the current situation due to medical, legal, philosophical and also ethical and religious arguments. Therefore, a decision for or against the COVID19 vaccination must be made individually.
The rationale for our position is summarized in seven arguments. They are consistent with the positions of thousands of scientists in Austria, Switzerland, Italy, France, Scandinavia, Great Britain and the United States.
1st argument: The pandemic with SARS-CoV2 will not be ended by vaccination
One goal of the general compulsory vaccination is to create a population immunized against SARS-CoV2. We consider it questionable whether this goal can actually be achieved with the vaccines available, which are still conditionally approved in the EU.
1.) The immunization by the current vaccines is much weaker and shorter lasting than expected and promised. At most, there is self-protection against severe courses and that only for a few months.
2.) These vaccines do not produce 'sterile' immunity. Despite vaccination, infections and the transmission of viruses are possible at any time. The extent and duration of the external protection are unknown.
3.) New virus variants bypass vaccination protection more and more successfully. The development and vaccination of a vaccine adapted to new virus variants will, according to the current state of affairs, take longer than the average time interval between the appearance of more successful variants. Consequently, this reactive vaccine adaptation cannot produce a uniformly immunized population.
4.) The evolutionary logic of the virus mutation is that of the new variants, those who best bypass the protection of the existing vaccines will be most successful. Full vaccination of the population - with vaccination that does not produce sterile immunity - can increase selection pressure on the virus and therefore even be counterproductive.
2nd argument: The risk potential of the vaccines is too high
Since the start of the vaccination campaign, no systematic research - including the long-term - risk potential of the novel vaccines has taken place. For the gene-based COVID19 vaccines, it is particularly important that the vaccines and their modes of action are fundamentally new and have not been researched in long-term studies. Vaccine damage could occur in a different way than experience with conventional vaccines suggests.
1.) Even the suspected cases of side effects from COVID19 vaccination recorded by the Paul Ehrlich Institute are worrying in relation to reports on other vaccines. Systematic research into side effects and risk factors associated with vaccinations is therefore urgently required.
2.) In addition, the current research shows warning signs of a considerable risk potential of these vaccines:
a) In 2021, and especially in the last few months, there was a significant increase in excess mortality, which has parallels to vaccination: if the number of vaccinations increases, excess mortality also increases; if the number of vaccinations decreases, excess mortality also decreases. This pattern can be found in various countries and could possibly be an indication of previously overlooked dramatic side effects (Appendix 1).
b) The unusually strong increase in cardiovascular and neurological diseases since the start of the vaccination campaign also shows parallels to the vaccination curves (Appendix 2).
c) There are indications that the indicators of the risk of infarction that can be detected in the blood increase significantly after vaccination.
d) The effect of the spike proteins on the human cell metabolism is largely not understood. There is serious evidence that it can be a cause of undesirable side effects.
e) Research results indicate that these side effects can be individual and deviate from the previously known patterns.
f) Current findings on the Omikron variant indicate that people vaccinated against an earlier variant are more susceptible to this new variant than non-vaccinated people.
3rd argument: The risk potential of multiple administration of SARS-CoV-2 vaccinations has not been adequately researched
The vaccination requirement will presumably provide for continued booster vaccinations, as vaccination protection decreases rapidly and new virus variants emerge. The multiple vaccination (more than two) is an ongoing experiment on the population to accumulate vaccination risks. Then:
1.) So far, no data has been collected in the manufacturer's approval studies.
2.) Also in connection with the currently running booster campaigns, hardly any comprehensive analyzes on the security of the procedure have been published.
4th argument: The general compulsory vaccination with the currently conditionally approved COVID19 vaccines violates constitutional law
The guarantee of human dignity in Article 1 of the Basic Law is the basis of the Basic Law: As an end-to-end being, the human being is the foundation and goal of law. State measures must never treat it as a mere means to an end (be it for the common good). The dignity of the individual subject cannot be weighed against other fundamental rights; it is rather absolute. An obligation to vaccinate interfered with the protection of the right to self-determination, guaranteed by the guarantee of human dignity, with regard to medical interventions in the physical and mental integrity and in the physical integrity of the person concerned, which is protected by Article 2, Paragraph 2 of the Basic Law. Furthermore, an impairment of the freedom of belief and conscience according to Art. 4 GG is possible.
1.) With regard to the encroachment on Article 2, Paragraph 2 of the Basic Law, the constitutionality of an obligation to vaccinate is questionable because of the questionable purpose and lack of suitability , necessity and appropriateness .
a) In this respect, the choice of a legitimate purpose is unclear . The main considerations are: herd immunity, interruption of chains of infection, avoidance of deaths and severe courses (and the associated relief for the health system), end of the pandemic.
b) The suitability of a general compulsory vaccination is clearly denied with regard to the first two purposes mentioned under a). With a view to avoiding severe courses, it should be pointed out that the conditionally approved vaccines lose their effect after a very short period of time (3 to 6 months) and, in any case, are not suitable for the long term. Furthermore, their effectiveness for new virus mutations cannot be assumed (cf. 1st argument under 3.). For the same reasons, a general compulsory vaccination is also unsuitable for ending the pandemic.
c) The necessity would only be answered in the affirmative if there were no more lenient means of achieving the goals that would be equally suitable. Since the suitability is questionable, considerations are at best hypothetical: Such considerations would, for example, concern the protection of vulnerable groups, the improvement of the health system or the (if possible) prompt adaptation of the vaccines. In the design of the general vaccination obligation, less drastic variants should also be considered: for example, a wide exemption for medical indications even in the case of existing medical uncertainties (autoimmune diseases, dispositions for vaccine damage - previous allergies or damage to vaccinations, known heart diseases, etc.), which an individual Enable doctor-patient weighing.
d) Appropriatenessin the narrower sense presupposes that when weighing up the impaired and the protected interests, there is a clear predominance of the protection of the general public intended by the mandatory vaccination. That is not the case here. Because the risk ratio between the risk of a severe course or death from COVID and the risk of severe or fatal side effects from the vaccination is to the disadvantage of the vaccination for large groups of people. According to serious scientists, the risk of younger adults is higher in the case of vaccination. In addition, there is a demonstrably considerable risk potential of the new and only conditionally approved vaccines, which is not yet sufficiently well known (cf. 2nd argument). That means,
2.) A mandatory vaccination subject to a fine collides with Art. 1 GG. This protectspeople from being reified - treated as a mere object. Due to the obligation to vaccinate, he would be forced to tolerate an irreversible intervention in his body through a medical treatment that was previously only conditionally approved, i.e. a medical treatment complex that has not yet been adequately researched. This would also be done solely for the sake of the other members of society or for the purpose of fighting pandemics for society as a whole or - depending on the target - to maintain medical treatment resources. To what extent these purposes can actually be achieved through compulsory vaccination is unclear. What is constitutionally clear, however, is that the use of the individual is inadmissible even if if it can protect the well-being and even the lives of many others with a probability bordering on certainty. Unvaccinated people in their sheer existence would be made illegal by a general obligation to vaccinate and criminalized by the threat of sanctions.
3.) With regard to Article 4 of the Basic Law, it should be borne in mind that individuals are free to refuse medical interventions for ideological or religious reasons in the area of their freedom of belief and conscience.
5th argument: The overload of the hospitals by COVID19 sufferers is not clearly proven by the statistical data
The general compulsory vaccination is justified, among other things, by relieving the burden on hospitals and in particular on intensive care units. There are also many unanswered questions in this context.
1.) Even after almost two years of pandemic, there are no reliable findings as to what proportion of the reported COVID19 patients are being treated in hospitals for a COVID19 disease and what proportion is in the hospital for another cause.
2.) Insufficient statistical information is available on the vaccination status, age distribution and the presence of previous illnesses of the actual COVID19 patients.
3.) Hospitals are subject to economic constraints and political incentives when providing treatment capacities for COVID-19. Ongoing debates about the decreasing number of beds registered as "operable" under changing framework conditions lead to the question: Can the burden on this system not be relieved through appropriate and transparent administrative and financial support?
6th argument: Measures other than vaccination have not been exhausted
The one-sided propagation of the compulsory vaccination continues the neglect of other effective measures against the pandemic that has already been practiced in the past two years, such as the failure to improve the working conditions of nurses and doctors, the maintenance or replenishment of intensive care bed capacity, and the development and use of therapies and Medication.
7th argument: The COVID19 vaccination requirement accelerates social conflicts
The compulsory vaccination is based on the assumption that society can return to normal with it. The opposite is the case: society is being divided more deeply. Citizens who consciously decide against vaccination for medical, ideological, religious or other reasons are marginalized and possibly even prosecuted. Public discourse creates artificial worlds in which critical voices can hardly be heard. Language itself is also pushed into the role of a vicarious agent for controversial political goals. Simplifying definitions (“vaccinated” - “unvaccinated”) promote polarization in our society; Euphemistic abbreviations such as “2-G” disguise the fact that a (large) minority is systematically, publicly and rigidly excluded from social life.
As a result of the growing politicization, there is also an interdisciplinary ideological standardization in academic research as “science”. This represents a disregard for the plural, free discourse on the urgently needed gain in knowledge about the benefits and risks of vaccination.
The confidence of many citizens in the state could be fundamentally shaken by strengthening this course. The resulting conflicts affect the rule of law and democracy.
The seven arguments put forward are intended to raise questions, the clarification of which should be a prerequisite for a decision regarding compulsory vaccination against Covid-19.
The arguments are not directed against a specific content position. Rather, they are arguments in favor of the fact that in the current situation it is important to develop a common approach to questions in science that allows a currently non-existent solid basis to be found for health and mental distress with a view to all dimensions of the crisis to alleviate with each other.
Out of this spirit of freedom of science and human dignity, we ask that joint efforts be made to overcome the current situation with its multiple suffering and the division of our society and to heal its scars permanently.
Investments
Attachment 1:
a) Germany: Course of excess mortality (Euromomo) and course of the three vaccinations per week:
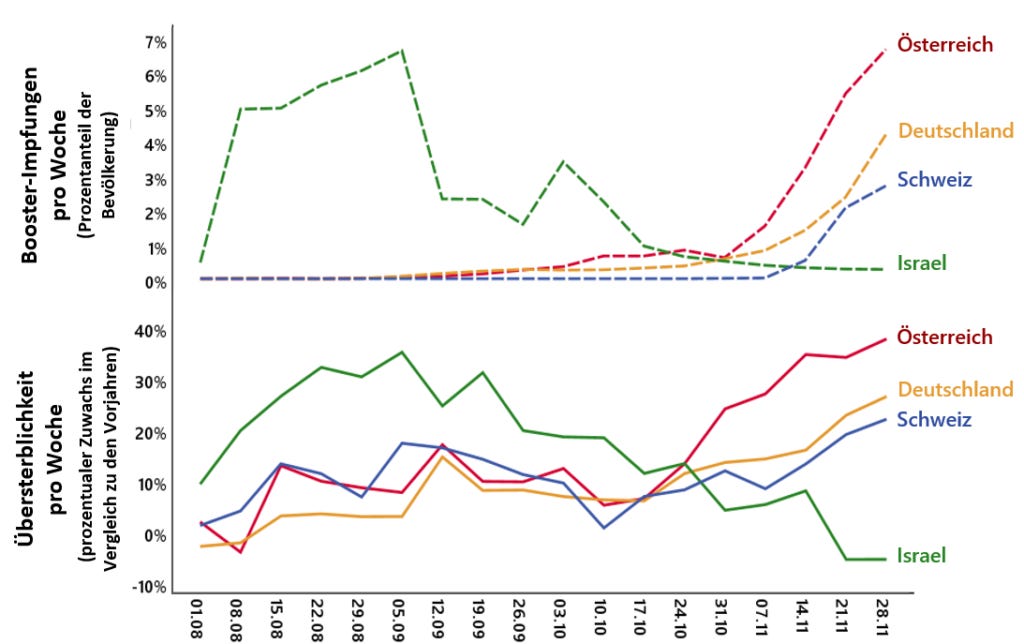
b) Country comparison: Course of excess mortality and course of booster vaccinations per week in Germany, Israel, Austria and Switzerland:
Treatments for respiratory diseases are diverse. Typical standard treatment methods have been suppressed by the covid paradigm by protocol dictate from health authorities. That suppression must stop. This is a general argument. Known treatments are myriad and “vaccinate every blade of grass and living soul instead of treating the sick” is a reckless unfounded spiral into the psychotic abyss that must end with a return to sensible medicine: treat the sick.
This is not just an argument for ivermectin, or for any of the other smeared low cost treatments (ivermectin costs about 0.01 USD per dose to produce). It’s an argument for treatment in general. But I see no reason to exclude ivermectin:
Results of the world’s largest study of ivermectin in COVID have just been posted. Meticulously collected data from hundreds of thousands of patients find massive reductions in hospitalization & death. “Controversy” over. Join us tomorrow for discussion with study investigators
FLCCC—Front Line COVID-19 Critical Care Alliance
This Wednesday at 7 p.m. ET four leading doctors—Dr. Kory, Dr. Marik, Dr. Kerr, and Dr. Cadegiani—discuss definitive results from the largest study of IVM in COVID-19, proving it an unequivocal public health game changer. Register here:
You can take a covid mRNA “vaccine” injection every single month instead if you prefer, as certain health ministers apparently prefer, not just for the sick, but for everyone:
I have trouble watching anything where everyone is muzzled in face diapers to begin with, a spiral into the psychotic abyss. Are doctors and nurses supposed to believe that we don’t live in a world of viruses? That living beings don’t deal with viruses? That this virus bounces off masks? That respiratory disease is not common? That treatment for the sick doesn’t work? That magical jabs for every living soul are “the only tool”?
Wow! Have a look at this article by the Danish Daily Extra Bladet (use google translate): what it basically says is that not only the authorities, but also media have COMPLETELY FAILED in their coverage of the pandemic! Instead of presenting TRUE, TRUTHFUL and REPRESENTATIVE information about Covid and the pandemic, authorities and media have pushed hysteria, fear, and panic, presenting a false narrative regarding the severity and impact of Covid.
Cudos to Extrablader for being first in admitting that media have not done their job.
Are you interested in reading journalists, scientists, statisticians, doctors and others who’ve been doing serious research on this? Here are some I’ve read recently:
“Where’s the vaccine mandate they promised us?” whines Daniel Brössler, reporter for the Süddeutsche Zeitung, disappointed because yesterday’s Corona summit of German minister presidents returned nothing but some adjustments to quarantine and sharpened testing rules. The double vaccinated will now have to submit negative tests if they want to eat at restaurants. Markus Söder, lockdown- and vaccine mandate-loving minister president of Bavaria, criticised even these milquetoast restrictions, with some bluster about how he’d already taken a hard line against bars and discos. This is after leading German Corona astrologer, Christian Drosten, used his state media podcast to suggest that Germany should start tolerating some of degree of SARS-2 transmission, and that breakthrough infections among the vaccinated should be considered normal. Such statements, which almost surely reflect sentiments within the coalition government, destroy most of the rationale for ongoing restrictions and vaccine mandates.
Meanwhile, in Austria, the thrice-vaccinated chancellor Karl Nehammer has tested positive for Corona. The news comes as Austria announces they will delay implementing their vaccine mandate by two months. It will now take effect in April, if at all. Gerald Gartlehner, an epidemiologist and sometime governmental adviser, suggested that mandates (or at least their enforcement) might have to be re-evaluated in light of Omicron and the widespread immunity the new variant will elicit across the Austrian population. There is every reason to think that Austria will be past the peak of the Omicron wave in April, and that a majority of Austrians with have SARS-2 antibodies by then.
It is obvious that we are at a turning point, even if everyone has yet to realise it – even if France is sharpening vaccine requirements, even if Italy has imposed vaccine mandates for everyone over 50, and even if Canada is for the moment determined to remain a prison state. This is the first time since the Floyd riots in America, that major political leaders and public health authorities have said that preventing Corona can no longer be the highest goal of western society.
It is a commonplace observation, but a true one: Since the vaccines began to fail in August, the vaccinators have been progressing through the proverbial five stages of grief. They spent a lot of time in denial, before becoming very angry and punitive. Then they began bargaining, hoping that SARS-2 would go away after four doses, or after five, with just the right dosing intervals, with a return to double masking, with child vaccinations. Now they appear to be drifting finally into depression and acceptance. They have realised, not a second too soon, that there is nothing to be done.
Omicron is a highly contagious variant with immune escape features. The vaccinators can vaccinate all they want, but their vaccines will not stop the waves of infection to come. A lot of the hyperbolic rhetoric about Corona was put about in the hopes that the most everyone wouldn’t be infected. They thought they could terrify people for a few years, vaccinate them, and harvest their gratitude for saving them from the worst respiratory virus since SARS. Now, though, it it is clear that everyone will have personal experience with Corona infection, whether or not they are vaccinated. This will destroy popular faith in measures, it will erode confidence in the vaccines, and it will do away with fear of the virus. Maybe a few people somewhere will still support containment, after two years of heavy restrictions, mandated vaccinations, and personal experience with infection, but I doubt there will be very many of them. It’s the beginning of the end.
Reflections on the Supreme Court oral arguments in the OSHA vaccine mandate case
Everything the Democratic appointees know about the pandemic comes from the TV and it's entirely wrong
I listened to the oral arguments this morning in connection with the OSHA vaccine mandate case. I found the whole experience depressing to the point where it is difficult to even write about it without losing my mind. Even if we win and this totalitarian government overreach is struck down, I fear for the future of our country…
In considering the aggressive lobbying for the introduction of vaccine passports, we would do well to remember and reflect on the following quote by French philosopher, author and journalist, Albert Camus (Homage to an exile, 1955): "Le bien-être du peuple en particulier a toujours été l’alibi des tyrans, et il offre de plus l’avantage de donner bonne conscience aux domestiques de la tyrannie" (The well-being of the people in particular has always been the alibi of tyrants and it offers the additional advantage of giving the servants of tyranny a good conscience).
The case put forward for the introduction of covid vaccine passports rests on a single premise: that covid vaccination reduces the risk of onward transmission of the virus by vaccinated individuals - we know from several studies and clinical evidence that this is categorically not the case as the vaccines do not neutralise susceptibility or transmissibility.
The United Kingdom Health Security Agency's (UKHSA) regular vaccine surveillance reports have shown that vaccinated individuals are more likely to be infected with covid than unvaccinated individuals. Their most recent report shows that, in most age groups (18 to 69 year olds), vaccinated people are about twice as likely to be PCR positive than unvaccinated individuals. These figures are more or less in line with the United Kingdom's Office of National Statistics' (ONS) contemporary prevalence estimates of around one in 50, or 2%, of the population, or 200 of 10,000 people, being infected.
There is quite simply no case for the introduction of vaccine passports other than a nefarious one.
(Sources regarding susceptibility and transmissibility for the vaccinated vs the unvaccinated:
By Elizabeth Lee Vliet, M.D. and Ali Shultz, J.D. –
https://www.truthforhealth.org/
Upon admission to a once-trusted hospital, American patients with COVID-19 become virtual prisoners, subjected to a rigid treatment protocol with roots in Ezekiel Emanuel’s “Complete Lives System” for rationing medical care in those over age 50. They have a shockingly high mortality rate. How and why is this happening, and what can be done about it?
As exposed in audio recordings, hospital executives in Arizona admitted meeting several times a week to lower standards of care, with coordinated restrictions on visitation rights. Most COVID-19 patients’ families are deliberately kept in the dark about what is really being done to their loved ones.
The combination that enables this tragic and avoidable loss of hundreds of thousands of lives includes (1) The CARES Act, which provides hospitals with bonus incentive payments for all things related to COVID-19 (testing, diagnosing, admitting to hospital, use of remdesivir and ventilators, reporting COVID-19 deaths, and vaccinations) and (2) waivers of customary and long-standing patient rights by the Centers for Medicare and Medicaid Services (CMS).
In 2020, the Texas Hospital Association submitted requests for waivers to CMS. According to Texas attorney Jerri Ward, “CMS has granted ‘waivers’ of federal law regarding patient rights. Specifically, CMS purports to allow hospitals to violate the rights of patients or their surrogates with regard to medical record access, to have patient visitation, and to be free from seclusion.” She notes that “rights do not come from the hospital or CMS and cannot be waived, as that is the antithesis of a ‘right.’ The purported waivers are meant to isolate and gain total control over the patient and to deny patient and patient’s decision-maker the ability to exercise informed consent.”
Creating a “National Pandemic Emergency” provided justification for such sweeping actions that override individual physician medical decision-making and patients’ rights. The CARES Act provides incentives for hospitals to use treatments dictated solely by the federal government under the auspices of the NIH. These “bounties” must paid back if not “earned” by making the COVID-19 diagnosis and following the COVID-19 protocol.
The hospital payments include:
A “free” required PCR test in the Emergency Room or upon admission for every patient, with government-paid fee to hospital.
Added bonus payment for each positive COVID-19 diagnosis.
Another bonus for a COVID-19 admission to the hospital.
A 20 percent “boost” bonus payment from Medicare on the entire hospital bill for use of remdesivir instead of medicines such as Ivermectin.
Another and larger bonus payment to the hospital if a COVID-19 patient is mechanically ventilated.
More money to the hospital if cause of death is listed as COVID-19, even if patient did not die directly of COVID-19.
A COVID-19 diagnosis also provides extra payments to coroners.
CMS implemented “value-based” payment programs that track data such as how many workers at a healthcare facility receive a COVID-19 vaccine. Now we see why many hospitals implemented COVID-19 vaccine mandates. They are paid more.
Outside hospitals, physician MIPS quality metrics link doctors’ income to performance-based pay for treating patients with COVID-19 EUA drugs. Failure to report information to CMS can cost the physician 4% of reimbursement.
Because of obfuscation with medical coding and legal jargon, we cannot be certain of the actual amount each hospital receives per COVID-19 patient. But Attorney Thomas Renz and CMS whistleblowers have calculated a total payment of at least $100,000 per patient.
What does this mean for your health and safety as a patient in the hospital?
There are deaths from the government-directed COVID treatments. For remdesivir, studies show that 71–75 percent of patients suffer an adverse effect, and the drug often had to be stopped after five to ten days because of these effects, such as kidney and liver damage, and death. Remdesivir trials during the 2018 West African Ebola outbreak had to be discontinued because death rate exceeded 50%. Yet, in 2020, Anthony Fauci directed that remdesivir was to be the drug hospitals use to treat COVID-19, even when the COVID clinical trials of remdesivir showed similar adverse effects.
In ventilated patients, the death toll is staggering. A National Library of Medicine January 2021 report of 69 studies involving more than 57,000 patients concluded that fatality rates were 45 percent in COVID-19 patients receiving invasive mechanical ventilation, increasing to 84 percent in older patients. Renz announced at a Truth for Health Foundation Press Conference that CMS data showed that in Texas hospitals, 84.9% percent of all patients died after more than 96 hours on a ventilator.
Then there are deaths from restrictions on effective treatments for hospitalized patients. Renz and a team of data analysts have estimated that more than 800,000 deaths in America’s hospitals, in COVID-19 and other patients, have been caused by approaches restricting fluids, nutrition, antibiotics, effective antivirals, anti-inflammatories, and therapeutic doses of anti-coagulants.
We now see government-dictated medical care at its worst in our history since the federal government mandated these ineffective and dangerous treatments for COVID-19, and then created financial incentives for hospitals and doctors to use only those “approved” (and paid for) approaches.
Our formerly trusted medical community of hospitals and hospital-employed medical staff have effectively become “bounty hunters” for your life. Patients need to now take unprecedented steps to avoid going into the hospital for COVID-19.
Covid has become a religion. Like, for example, Christianity, Covid now has its symbols and rituals: vaccination is like baptism, the face mask and the vaccine certificate are like the cross many Christians wear around their necks, and “follow the science!” is the Covid believers’ equivalent of prayer. Although science shows that these symbols / rituals are, like their Christian counterparts, not very functional.
This appears to have been a clarification to the backlash from people who completely misconstrued her statement that over 75% of people who are dying from Omicron had four or more comorbidities.
Some have taken this to mean that Walensky thinks that people who are disabled are not worthy of saving from COVID-19, a clear distortion of her language and meaning.
My disabled life is worthy’: CDC prompts backlash for comments on Omicron deaths
This position conflates “medical co-morbidities” with “disabilities”. People w/pre-existing medical conditions, who are “unwell to begin with”, do not automatically fall into the “disabled” category. That said, many people who are disabled are also immunocompromised.
The reality is that most deaths from COVID-19 have been in the elderly and in people w/co-morbidities from the beginning; early on, it was clear that >90% of deaths in Italy were in people who had pre-existing medical conditions.
Walensky is not saying she’s encouraged that the death risk with Omicron is strongly biased toward people with four or more comorbidities; she’s celebrating that the risk is not high in people with 3, 2, 1 and 0 comorbidities. She’s saying it’s mild for most people. (Sames was true for every other form of COVID-19, but that’s not what’s happening here.)
The backlash to her comments forced Walensky’s hand to state that the CDC is, in fact, going to “protect people with comorbidities from severe COVID-19”.
Her statement, “CDC is taking steps to protect those at highest risk, incl. those w/ chronic health conditions, disabilities & older adults” is in keeping with a public health policy that engages with the facts.
Astute denizens of Twitter, however, took note that Walensky did not provide any specifics on CDC’s plan to “protect people with comorbidities from severe COVID-19”.
Ivermectin for COVID-19: real-time meta analysis of 73 studies
10:51 AM · Jan 10, 2022
3 Reposts · 4 Likes
I then peppered responses to her tweet from people saying “you have abandoned my child” with invitations to ask an ethical physician about the science on early, aggressive treatments.
Let’s hope the people who feel abandoned can benefit from the hard work of ethical physicians.